💊 medicine
Acute Respiratory Distress Syndrome Clinical Features Diagnosis and Management Guide
Comprehensive and clinically structured guide on acute respiratory distress syndrome covering definition, pathophysiology, causes, Berlin diagnostic criteria, investigations, ventilatory strategies, ICU management, complications, prognosis, and prevention for medical students and clinicians.
Choose Your Mode
How do you want to practice?
Study Mode
Learn at your own pace. Get instant feedback and detailed explanations after each question.
Start Studying
Exam Mode
Simulate real exam conditions. Timed questions, full scoring, and performance breakdown.
Take Exam
Strict Exam
Maximum difficulty. Full-screen, no backtracking, strict timing. For serious preparation.
Frequently Asked Questions
❓ What is Acute Respiratory Distress Syndrome (ARDS)?
Acute Respiratory Distress Syndrome is a severe form of acute hypoxemic respiratory failure caused by diffuse inflammatory injury to the alveolar–capillary membrane, leading to non-cardiogenic pulmonary edema, decreased lung compliance, and refractory hypoxemia.
❓ What are the most common causes of ARDS?
The most common causes include sepsis (most frequent), severe pneumonia, aspiration of gastric contents, trauma, acute pancreatitis, massive blood transfusion (TRALI), inhalational injury, and near drowning.
❓ How is ARDS diagnosed?
ARDS is diagnosed using the Berlin criteria, which require acute onset within one week, bilateral pulmonary opacities on imaging, respiratory failure not explained by cardiac causes or fluid overload, and impaired oxygenation assessed by PaO2/FiO2 ratio with PEEP ≥5 cm H2O.
❓ How is ARDS severity classified?
ARDS severity is classified based on PaO2/FiO2 ratio: mild (200–300), moderate (100–200), and severe (<100), all measured with PEEP ≥5 cm H2O.
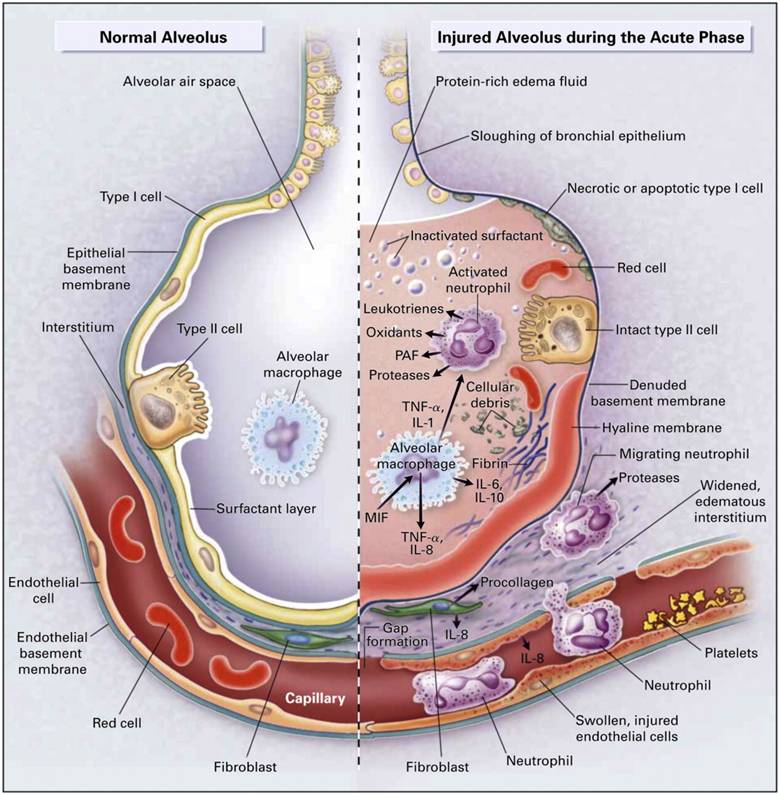
❓ What is the hallmark pathophysiology of ARDS?
The hallmark is diffuse alveolar damage resulting in increased capillary permeability, protein-rich alveolar edema, surfactant dysfunction, alveolar collapse, ventilation–perfusion mismatch, and refractory hypoxemia.
❓ How is ARDS different from cardiogenic pulmonary edema?
ARDS is characterized by non-cardiogenic pulmonary edema with normal left ventricular filling pressures, whereas cardiogenic pulmonary edema results from heart failure with elevated cardiac filling pressures.
❓ What is the cornerstone of ARDS management?
The cornerstone of ARDS management is lung-protective mechanical ventilation using low tidal volumes (6 mL/kg predicted body weight) and limiting plateau pressures to less than 30 cm H2O.
❓ Why is low tidal volume ventilation important in ARDS?
Low tidal volume ventilation reduces ventilator-induced lung injury, decreases alveolar overdistension, and has been proven to reduce mortality in ARDS patients.
❓ What role does PEEP play in ARDS management?
Positive end-expiratory pressure prevents alveolar collapse, improves oxygenation, reduces shunt, and helps maintain functional residual capacity in ARDS.
❓ When is prone positioning indicated in ARDS?
Prone positioning is indicated in moderate to severe ARDS (PaO2/FiO2 <150) and should be applied for at least 16 hours per day to improve oxygenation and survival.
❓ Is permissive hypercapnia allowed in ARDS?
Yes, permissive hypercapnia is allowed to maintain lung-protective ventilation, provided there are no contraindications such as raised intracranial pressure or severe metabolic acidosis.
❓ What is the role of neuromuscular blockers in ARDS?
Short-term neuromuscular blockade may be used in early severe ARDS to improve ventilator synchrony, reduce oxygen consumption, and improve oxygenation.
❓ Are corticosteroids useful in ARDS?
Corticosteroids may be beneficial in early moderate to severe ARDS to reduce inflammation and duration of mechanical ventilation, though timing and patient selection are important.
❓ What fluid strategy is recommended in ARDS?
A conservative fluid management strategy is recommended once shock has resolved, as it improves lung function and reduces ventilator days without increasing organ failure.
❓ When should ECMO be considered in ARDS?
Extracorporeal membrane oxygenation should be considered in severe ARDS with refractory hypoxemia despite optimal lung-protective ventilation, prone positioning, and neuromuscular blockade.
❓ What are common complications of ARDS?
Common complications include ventilator-associated pneumonia, barotrauma such as pneumothorax, multi-organ dysfunction, ICU-acquired weakness, and long-term pulmonary fibrosis.
❓ What is the mortality rate of ARDS?
The overall mortality rate ranges from 30 to 45 percent and increases with disease severity, advanced age, sepsis as the underlying cause, and presence of multi-organ failure.
❓ Can patients recover fully from ARDS?
Many patients recover good lung function, but some develop long-term sequelae such as reduced diffusion capacity, exercise intolerance, pulmonary fibrosis, and neurocognitive impairment.
❓ How can ARDS be prevented in ICU patients?
Prevention includes early treatment of sepsis, lung-protective ventilation in all mechanically ventilated patients, aspiration precautions, judicious fluid therapy, and avoidance of unnecessary blood transfusions.
❓ What is the most important prognostic factor in ARDS?
Severity of hypoxemia as measured by the PaO2/FiO2 ratio, along with the underlying cause and presence of multi-organ failure, are the most important prognostic factors.