💊 medicine
Aortic Regurgitation Comprehensive Guide Causes Symptoms Diagnosis Treatment
Aortic regurgitation explained in detail covering causes, pathophysiology, clinical features, diagnostic criteria, echocardiographic severity grading, medical management, surgical indications, and guideline-based treatment for acute and chronic aortic regurgitation.
Choose Your Mode
How do you want to practice?
Study Mode
Learn at your own pace. Get instant feedback and detailed explanations after each question.
Start Studying
Exam Mode
Simulate real exam conditions. Timed questions, full scoring, and performance breakdown.
Take Exam
Strict Exam
Maximum difficulty. Full-screen, no backtracking, strict timing. For serious preparation.
Frequently Asked Questions
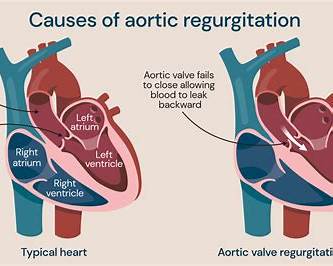
❓ What is aortic regurgitation?
Aortic regurgitation is a valvular heart disease in which blood flows back from the aorta into the left ventricle during diastole due to incomplete closure of the aortic valve.
❓ What are the main causes of aortic regurgitation?
Common causes include bicuspid aortic valve, rheumatic heart disease, infective endocarditis, aortic root dilation, Marfan syndrome, aortic dissection, and degenerative valve disease.
❓ What is the difference between acute and chronic aortic regurgitation?
Acute aortic regurgitation develops suddenly and causes severe pulmonary edema and hypotension, while chronic aortic regurgitation progresses slowly with left ventricular dilation and a long asymptomatic phase.
❓ What are the classic symptoms of chronic aortic regurgitation?
Symptoms include exertional dyspnea, fatigue, palpitations, angina, orthopnea, and paroxysmal nocturnal dyspnea, usually appearing late in the disease.
❓ Why does aortic regurgitation cause a wide pulse pressure?
Wide pulse pressure occurs due to increased systolic pressure from high stroke volume and decreased diastolic pressure from rapid blood runoff back into the left ventricle.
❓ What is the characteristic murmur of aortic regurgitation?
A high-pitched, early diastolic decrescendo murmur best heard along the left sternal border with the patient sitting forward.
❓ What is Austin Flint murmur?
Austin Flint murmur is a low-pitched mid-diastolic murmur at the apex caused by the regurgitant aortic jet interfering with mitral valve opening in severe aortic regurgitation.
❓ Which investigation is most important for diagnosing aortic regurgitation?
Echocardiography is the key investigation as it identifies the cause, grades severity, assesses left ventricular size and function, and evaluates the aorta.
❓ What echocardiographic finding strongly suggests severe aortic regurgitation?
Holodiastolic flow reversal in the descending aorta is a hallmark finding of severe aortic regurgitation.
❓ When is surgery indicated in asymptomatic severe aortic regurgitation?
Surgery is indicated when left ventricular ejection fraction is 55 percent or less, LV end-systolic dimension exceeds 50 mm, or indexed LVESD is greater than 25 mm per square meter.
❓ Why is surgery urgent in acute severe aortic regurgitation?
The left ventricle cannot adapt to sudden volume overload, leading to rapid pulmonary edema, cardiogenic shock, and high mortality without urgent valve replacement.
❓ Which drugs are useful in chronic aortic regurgitation?
Afterload-reducing agents such as ACE inhibitors, ARBs, and dihydropyridine calcium channel blockers are useful, especially in patients with hypertension or heart failure.
❓ Why is intra-aortic balloon pump contraindicated in aortic regurgitation?
Intra-aortic balloon pump increases diastolic pressure and worsens regurgitant flow back into the left ventricle.
❓ What is the role of cardiac MRI in aortic regurgitation?
Cardiac MRI is used when echocardiographic assessment is inconclusive, providing accurate measurement of regurgitant volume, regurgitant fraction, and ventricular volumes.
❓ What are the major complications of untreated severe aortic regurgitation?
Complications include irreversible left ventricular dysfunction, heart failure, arrhythmias, pulmonary hypertension, infective endocarditis, and increased mortality.