💊 medicine
High Altitude Pulmonary Edema and Hypothermia Clinical Features Diagnosis and Management
Comprehensive clinical guide on high altitude pulmonary edema and hypothermia covering definition, pathophysiology, risk factors, clinical features, diagnosis, differential diagnosis, emergency management, prevention strategies, complications, and exam-oriented pearls for medical students and clinicians.
Choose Your Mode
How do you want to practice?
Study Mode
Learn at your own pace. Get instant feedback and detailed explanations after each question.
Start Studying
Exam Mode
Simulate real exam conditions. Timed questions, full scoring, and performance breakdown.
Take Exam
Strict Exam
Maximum difficulty. Full-screen, no backtracking, strict timing. For serious preparation.
Frequently Asked Questions
❓ What is high altitude pulmonary edema?
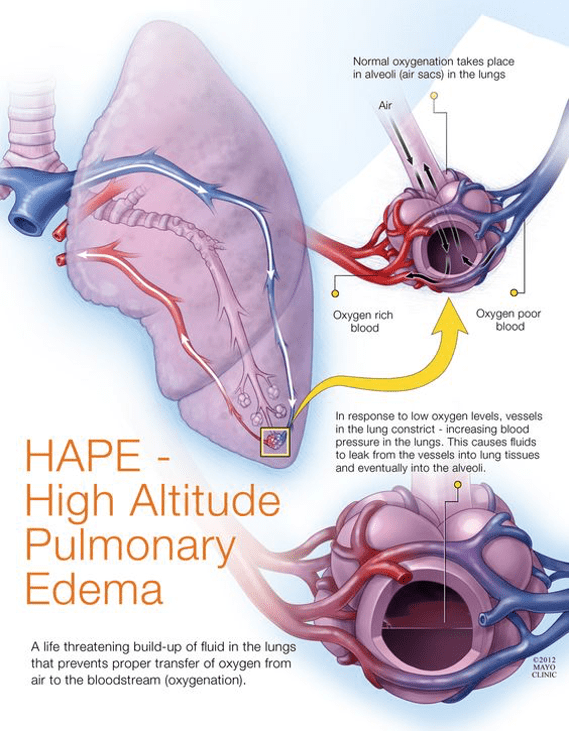
High altitude pulmonary edema is a life-threatening non-cardiogenic pulmonary edema caused by hypoxia-induced pulmonary hypertension after rapid ascent to high altitude, usually above 2500 to 3000 meters.
❓ What causes high altitude pulmonary edema?
It is caused by uneven hypoxic pulmonary vasoconstriction leading to high pulmonary artery pressure, capillary stress failure, and leakage of protein-rich fluid into the alveoli.
❓ What are the early symptoms of high altitude pulmonary edema?
Early symptoms include reduced exercise tolerance, exertional dyspnea, dry cough, fatigue, and mild chest tightness.
❓ What are the severe signs of high altitude pulmonary edema?
Severe signs include dyspnea at rest, orthopnea, pink frothy sputum, cyanosis, tachycardia, hypoxemia, and bilateral lung crackles.
❓ How is high altitude pulmonary edema diagnosed?
Diagnosis is primarily clinical based on symptoms, hypoxemia, chest findings, and history of recent ascent, supported by chest X-ray showing patchy bilateral infiltrates with normal heart size.
❓ What is the most important treatment for high altitude pulmonary edema?
Immediate descent to a lower altitude combined with supplemental oxygen is the most critical and life-saving treatment.
❓ Which medications are used in high altitude pulmonary edema?
Nifedipine is the primary drug used; phosphodiesterase-5 inhibitors like sildenafil may be used, and dexamethasone is added if cerebral edema is suspected.
❓ How can high altitude pulmonary edema be prevented?
Prevention includes gradual ascent, adequate acclimatization, avoiding strenuous exertion, keeping warm, and prophylactic nifedipine in individuals with prior HAPE.
❓ What is hypothermia?
Hypothermia is a condition in which core body temperature falls below 35 degrees Celsius due to excessive heat loss or impaired thermoregulation.
❓ How is hypothermia classified?
Hypothermia is classified as mild at 32 to 35 degrees Celsius, moderate at 28 to 32 degrees Celsius, and severe below 28 degrees Celsius.
❓ What are the common causes of hypothermia?
Common causes include environmental cold exposure, immersion in cold water, high altitude exposure, alcohol or sedative use, sepsis, hypothyroidism, and malnutrition.
❓ What are the clinical features of mild hypothermia?
Mild hypothermia presents with shivering, tachycardia, slurred speech, impaired coordination, and cold diuresis.
❓ What ECG change is characteristic of hypothermia?
Osborn or J waves on ECG are characteristic of hypothermia and indicate increased risk of ventricular arrhythmias.
❓ How is hypothermia managed?
Management includes gentle handling, airway and circulation support, correction of hypoglycemia, and rewarming using passive, active external, or active internal methods depending on severity.
❓ What is the principle behind resuscitation in hypothermia?
The key principle is that no one is considered dead until warm and dead, as hypothermia can mimic death and patients may recover after rewarming.