💊 medicine
Hyperaldosteronism Clinical Features Diagnosis and Management Guide
Comprehensive medical guide on hyperaldosteronism covering definition, causes, pathophysiology, clinical features, diagnostic approach, aldosterone renin ratio interpretation, differential diagnosis, and detailed stepwise management for students and clinicians.
Choose Your Mode
How do you want to practice?
Study Mode
Learn at your own pace. Get instant feedback and detailed explanations after each question.
Start Studying
Exam Mode
Simulate real exam conditions. Timed questions, full scoring, and performance breakdown.
Take Exam
Strict Exam
Maximum difficulty. Full-screen, no backtracking, strict timing. For serious preparation.
Frequently Asked Questions
❓ What is hyperaldosteronism?
Hyperaldosteronism is a condition characterized by excessive secretion of aldosterone from the adrenal cortex, leading to sodium and water retention, potassium loss, metabolic alkalosis, and hypertension.
❓ What are the main types of hyperaldosteronism?
The main types are primary hyperaldosteronism (autonomous aldosterone secretion with low renin), secondary hyperaldosteronism (renin-mediated aldosterone excess), and pseudohyperaldosteronism (aldosterone-like effects without high aldosterone).
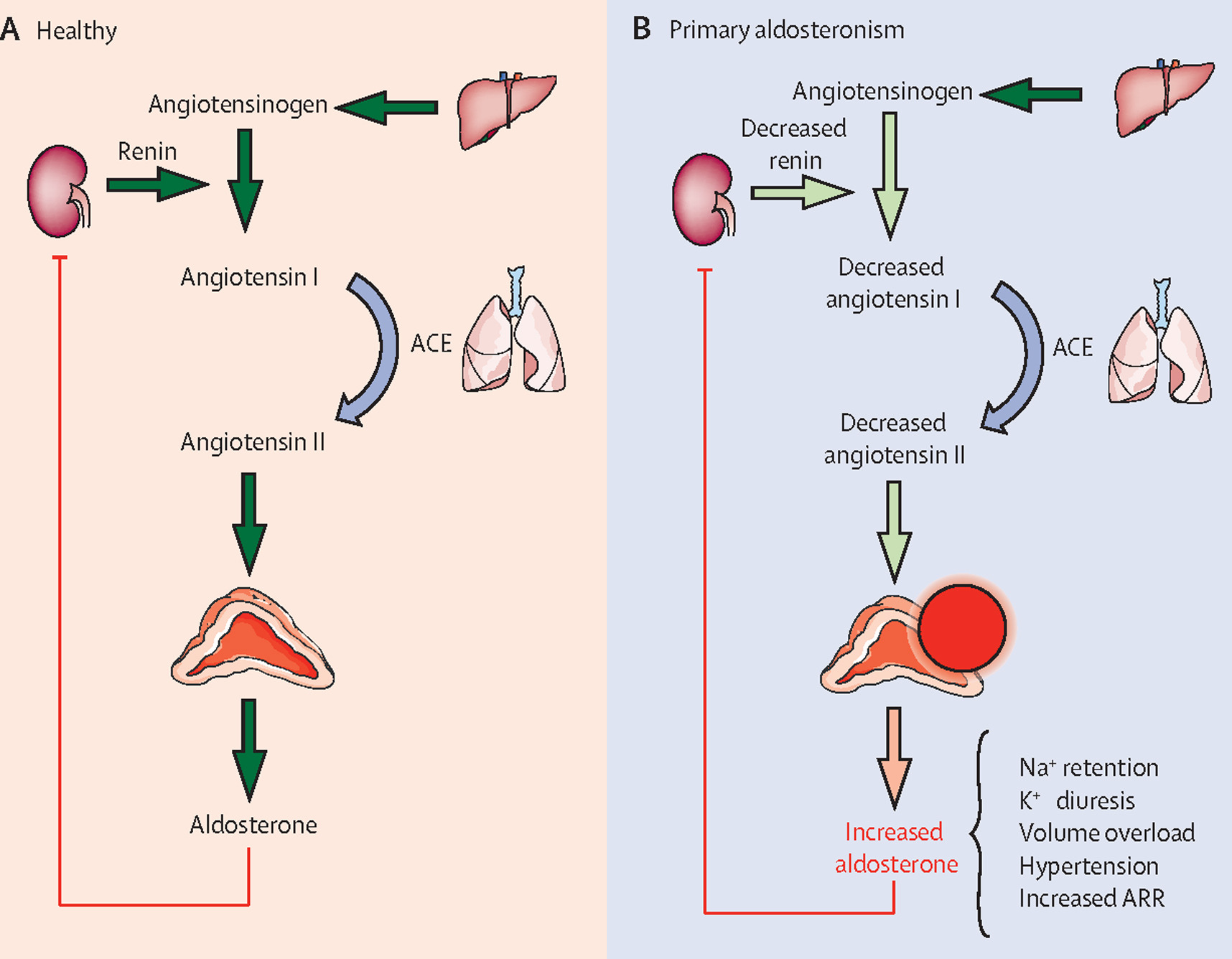
❓ What is primary hyperaldosteronism?
Primary hyperaldosteronism is caused by autonomous aldosterone production from the adrenal glands, most commonly due to aldosterone-producing adenoma or bilateral adrenal hyperplasia, with suppressed renin levels.
❓ What causes secondary hyperaldosteronism?
Secondary hyperaldosteronism results from increased renin secretion due to conditions such as renal artery stenosis, heart failure, cirrhosis, nephrotic syndrome, diuretic use, or pregnancy.
❓ What is Conn syndrome?
Conn syndrome refers to primary hyperaldosteronism caused by an aldosterone-producing adrenal adenoma.
❓ What are the common clinical features of hyperaldosteronism?
Common features include resistant hypertension, hypokalemia, muscle weakness, fatigue, polyuria, polydipsia, metabolic alkalosis, and increased cardiovascular risk.
❓ Is hypokalemia always present in hyperaldosteronism?
No, hypokalemia is not mandatory. Many patients with primary hyperaldosteronism have normal serum potassium levels, especially in early or mild disease.
❓ When should patients be screened for primary hyperaldosteronism?
Screening is recommended in resistant hypertension, hypertension with hypokalemia, adrenal incidentaloma with hypertension, early-onset hypertension, or family history of early stroke or hyperaldosteronism.
❓ What is the best initial screening test for primary hyperaldosteronism?
The plasma aldosterone–renin ratio (ARR) is the preferred initial screening test.
❓ How is primary hyperaldosteronism confirmed?
Confirmation is done using suppression tests such as saline infusion test, oral sodium loading test, fludrocortisone suppression test, or captopril challenge test.
❓ What is the role of adrenal venous sampling?
Adrenal venous sampling is the gold standard to differentiate unilateral from bilateral aldosterone secretion and is required before surgical intervention.
❓ How is unilateral primary hyperaldosteronism treated?
Unilateral disease is treated with laparoscopic adrenalectomy, which often normalizes potassium levels and improves or cures hypertension.
❓ How is bilateral adrenal hyperplasia managed?
Bilateral disease is managed medically using mineralocorticoid receptor antagonists such as spironolactone or eplerenone.
❓ What drugs are used to treat hyperaldosteronism?
Common drugs include spironolactone, eplerenone, and amiloride, depending on the cause and patient tolerance.
❓ What are the major complications of untreated hyperaldosteronism?
Complications include stroke, myocardial infarction, atrial fibrillation, left ventricular hypertrophy, chronic kidney disease, and increased cardiovascular mortality.
❓ Why does hyperaldosteronism not usually cause edema?
Aldosterone escape occurs due to pressure natriuresis and atrial natriuretic peptide, preventing persistent edema despite sodium retention.
❓ What acid–base abnormality is seen in hyperaldosteronism?
Metabolic alkalosis occurs due to increased hydrogen ion secretion in the renal tubules.
❓ What is familial hyperaldosteronism type I?
It is a glucocorticoid-remediable form of hyperaldosteronism caused by a genetic defect, where aldosterone secretion is regulated by ACTH and suppressed by low-dose glucocorticoids.
❓ What is the prognosis of hyperaldosteronism?
With early diagnosis and appropriate treatment, prognosis is excellent, with significant reduction in cardiovascular and renal complications.
❓ Can hyperaldosteronism be cured?
Yes, unilateral primary hyperaldosteronism can often be cured with adrenalectomy, while bilateral disease can be effectively controlled with medical therapy.