💊 medicine
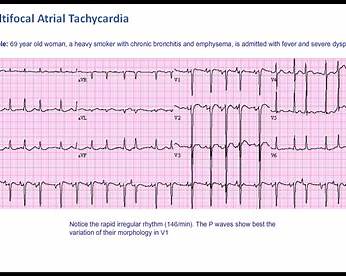
Multifocal Atrial Tachycardia Clinical Features ECG Diagnosis and Management
Multifocal atrial tachycardia explained in detail with definition, pathophysiology, causes, ECG diagnostic criteria, differential diagnosis, investigations, stepwise management, drug therapy, contraindications, prognosis, and exam-oriented clinical points for medical students and clinicians.
Choose Your Mode
How do you want to practice?
Study Mode
Learn at your own pace. Get instant feedback and detailed explanations after each question.
Start Studying
Exam Mode
Simulate real exam conditions. Timed questions, full scoring, and performance breakdown.
Take Exam
Strict Exam
Maximum difficulty. Full-screen, no backtracking, strict timing. For serious preparation.
Frequently Asked Questions
❓ What is multifocal atrial tachycardia (MAT)?
Multifocal atrial tachycardia is a supraventricular tachyarrhythmia characterized by an irregular rhythm, heart rate greater than 100 beats per minute, and at least three different P-wave morphologies on ECG, caused by multiple ectopic atrial pacemakers.
❓ What is the most common cause of multifocal atrial tachycardia?
The most common cause of multifocal atrial tachycardia is hypoxia, most frequently seen in patients with chronic obstructive pulmonary disease or acute pulmonary illnesses.
❓ How is multifocal atrial tachycardia diagnosed?
MAT is diagnosed on ECG by the presence of an irregularly irregular rhythm, heart rate over 100 per minute, at least three distinct P-wave morphologies, variable PR intervals, and an isoelectric baseline between P waves.
❓ How can multifocal atrial tachycardia be differentiated from atrial fibrillation?
MAT shows discrete P waves with different morphologies and an isoelectric baseline, whereas atrial fibrillation has no distinct P waves and shows continuous fibrillatory activity.
❓ What is wandering atrial pacemaker and how is it different from MAT?
Wandering atrial pacemaker has similar ECG features to MAT but the heart rate is less than 100 beats per minute, whereas MAT has a heart rate greater than 100 beats per minute.
❓ What is the most important step in managing multifocal atrial tachycardia?
The most important step is treatment of the underlying cause, such as correcting hypoxia, treating pulmonary disease, managing infection, and correcting electrolyte abnormalities.
❓ Which drugs are preferred for rate control in multifocal atrial tachycardia?
Magnesium sulfate and non-dihydropyridine calcium channel blockers such as verapamil or diltiazem are preferred for rate control in MAT.
❓ Are beta blockers recommended in multifocal atrial tachycardia?
Beta blockers are generally avoided or used cautiously because many MAT patients have underlying COPD or asthma, where beta blockers may worsen bronchospasm.
❓ Is electrical cardioversion effective in multifocal atrial tachycardia?
No, electrical cardioversion is ineffective in MAT because the arrhythmia is due to enhanced automaticity rather than a re-entrant mechanism.
❓ Does multifocal atrial tachycardia require anticoagulation?
No, anticoagulation is not indicated in multifocal atrial tachycardia as it does not increase the risk of thromboembolism.
❓ What electrolyte abnormalities are commonly associated with MAT?
Hypokalemia and hypomagnesemia are commonly associated with MAT and should be corrected promptly.
❓ Can digoxin be used to treat multifocal atrial tachycardia?
No, digoxin is generally ineffective in MAT and may worsen the arrhythmia due to increased atrial automaticity.
❓ What drugs can precipitate multifocal atrial tachycardia?
Drugs such as theophylline, beta-agonists, and excess catecholamines can precipitate or worsen MAT.
❓ What is the prognosis of multifocal atrial tachycardia?
The prognosis depends on the severity of the underlying illness; MAT itself is usually benign but is often a marker of severe systemic or pulmonary disease.
❓ In which patient population is multifocal atrial tachycardia most commonly seen?
MAT is most commonly seen in elderly patients with severe pulmonary disease, particularly chronic obstructive pulmonary disease.