📋 Paediatrics
Pediatric Malnutrition Causes, Types, Clinical Features and WHO Management
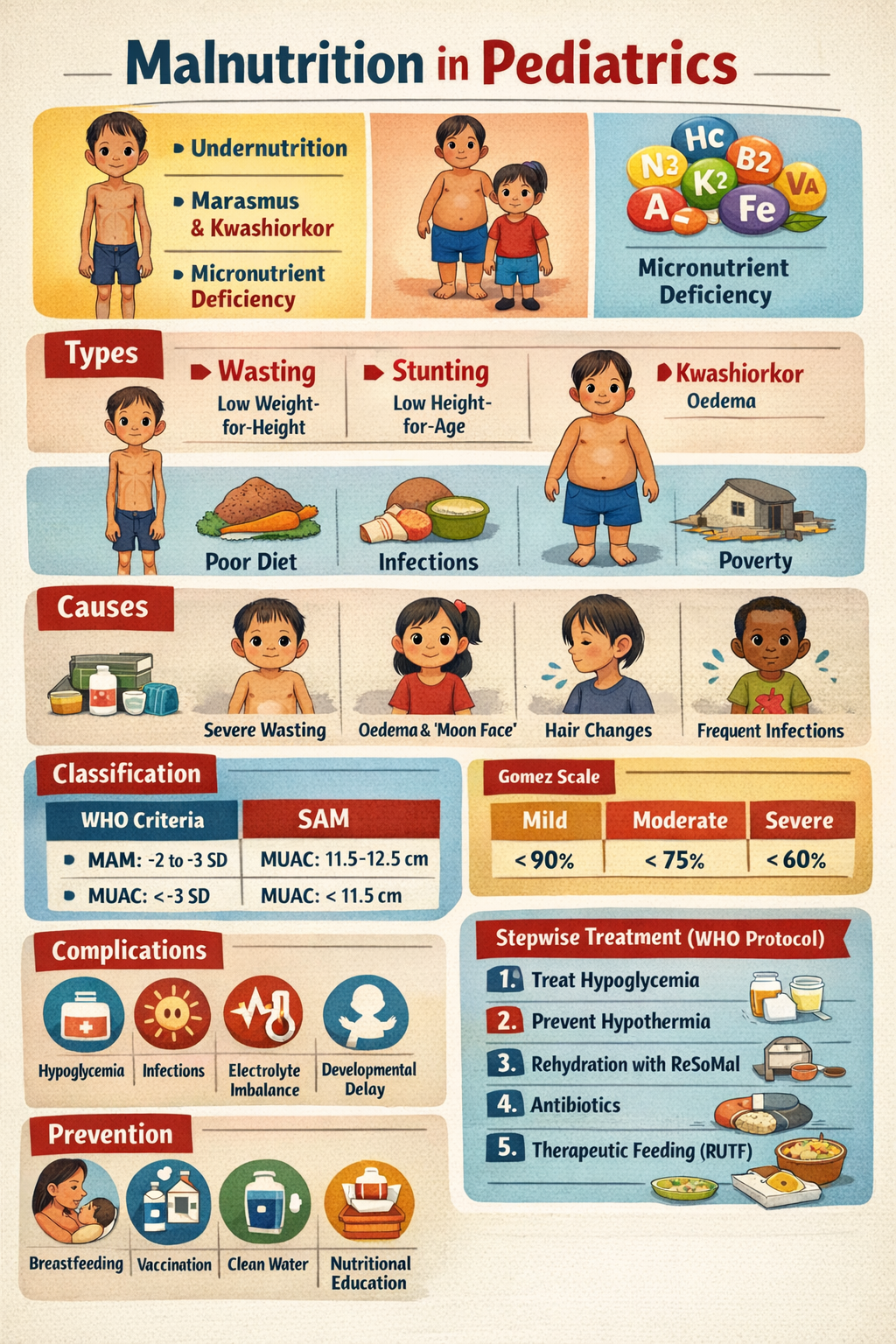
Learn complete details about pediatric malnutrition including causes, classification, marasmus and kwashiorkor differences, clinical signs, investigations, WHO stepwise treatment protocol, complications, and prevention strategies.
Choose Your Mode
How do you want to practice?
Study Mode
Learn at your own pace. Get instant feedback and detailed explanations after each question.
Start Studying
Exam Mode
Simulate real exam conditions. Timed questions, full scoring, and performance breakdown.
Take Exam
Strict Exam
Maximum difficulty. Full-screen, no backtracking, strict timing. For serious preparation.
Frequently Asked Questions
❓ What is malnutrition in pediatrics?
Malnutrition in pediatrics is a condition where a child has deficiency, excess, or imbalance of energy, protein, or micronutrients, leading to poor growth, impaired immunity, and developmental delay.
❓ What are the main types of pediatric malnutrition?
The main types are undernutrition (wasting, stunting, underweight), protein–energy malnutrition (marasmus, kwashiorkor), micronutrient deficiencies, and overnutrition (obesity).
❓ What is the difference between marasmus and kwashiorkor?
Marasmus is severe calorie deficiency causing wasting without edema, while kwashiorkor is primarily protein deficiency causing edema, fatty liver, and skin/hair changes.
❓ What is severe acute malnutrition (SAM)?
SAM is defined by weight-for-height Z score < –3 SD, MUAC < 11.5 cm, or the presence of bilateral pitting edema.
❓ What is moderate acute malnutrition (MAM)?
MAM is defined by weight-for-height Z score between –2 and –3 SD or MUAC between 11.5–12.5 cm without edema.
❓ What are the common causes of malnutrition in children?
Common causes include inadequate dietary intake, recurrent infections (diarrhea, pneumonia), poverty, food insecurity, poor breastfeeding, malabsorption disorders, and chronic illnesses.
❓ Why are infections common in malnourished children?
Malnutrition weakens the immune system, making children highly susceptible to infections and reducing their ability to mount fever responses.
❓ What are the clinical signs of kwashiorkor?
Kwashiorkor presents with bilateral edema, moon face, flaky paint dermatosis, sparse discolored hair (flag sign), hepatomegaly, apathy, and poor appetite.
❓ What are the clinical signs of marasmus?
Marasmus presents with severe wasting, loss of subcutaneous fat, an old-man appearance, no edema, and usually preserved appetite.
❓ What is MUAC and why is it important?
MUAC (Mid-Upper Arm Circumference) is a simple screening tool for acute malnutrition; MUAC < 11.5 cm indicates severe acute malnutrition.
❓ What is the first step in managing a child with SAM?
The first step is to treat life-threatening conditions such as hypoglycemia, hypothermia, dehydration, and infections before starting rehabilitation feeding.
❓ Why is hypoglycemia dangerous in malnutrition?
Hypoglycemia can rapidly lead to seizures, coma, and death in malnourished children due to low energy reserves.
❓ What is ReSoMal used for?
ReSoMal is a special oral rehydration solution used for dehydrated malnourished children because it contains less sodium and more potassium than standard ORS.
❓ Why is iron supplementation delayed in SAM treatment?
Iron is delayed until stabilization because it can worsen infections and increase oxidative stress during the acute phase.
❓ What is F-75 formula in SAM management?
F-75 is a starter therapeutic milk used in the stabilization phase; it provides low protein and low sodium calories to prevent refeeding syndrome.
❓ What is F-100 or RUTF used for?
F-100 and Ready-to-Use Therapeutic Food (RUTF) are used in the rehabilitation phase to promote rapid catch-up growth with high-energy feeding.
❓ What is refeeding syndrome?
Refeeding syndrome is a metabolic complication caused by sudden aggressive feeding, leading to electrolyte shifts such as hypophosphatemia, hypokalemia, edema, and arrhythmias.
❓ What are the major complications of severe malnutrition?
Complications include hypoglycemia, hypothermia, severe infections, electrolyte imbalance, heart failure, developmental delay, and increased mortality.
❓ How can pediatric malnutrition be prevented?
Prevention includes exclusive breastfeeding for 6 months, adequate complementary feeding, immunization, micronutrient supplementation, deworming, and improving sanitation and food security.