💊 medicine
Symptomatic Bradycardia With Pulse Management Guidelines and Drug Dosing
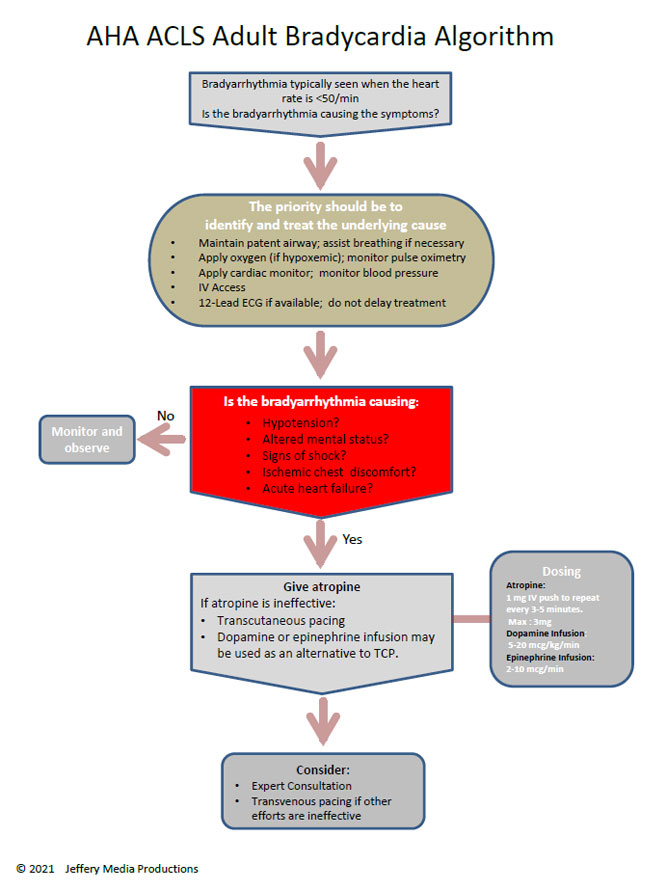
Comprehensive clinical guide on symptomatic bradycardia with pulse including causes, ECG diagnosis, ACLS management algorithm, atropine dosing, pacing indications, drug contraindications, and emergency treatment strategies.
Choose Your Mode
How do you want to practice?
Study Mode
Learn at your own pace. Get instant feedback and detailed explanations after each question.
Start Studying
Exam Mode
Simulate real exam conditions. Timed questions, full scoring, and performance breakdown.
Take Exam
Strict Exam
Maximum difficulty. Full-screen, no backtracking, strict timing. For serious preparation.
Frequently Asked Questions
❓ What is symptomatic bradycardia with a pulse?
Symptomatic bradycardia with a pulse is a clinical condition where the heart rate is abnormally slow, usually below 60 beats per minute, and the patient has a palpable pulse but develops symptoms such as hypotension, syncope, dizziness, altered mental status, chest pain, or signs of shock due to reduced cardiac output.
❓ What heart rate is considered dangerous in bradycardia?
There is no absolute heart rate cutoff, but rates below 50 beats per minute, and especially below 40 beats per minute, are more likely to cause symptoms and hemodynamic instability, particularly in elderly patients or those with structural heart disease.
❓ What are the common causes of symptomatic bradycardia?
Common causes include sinus node dysfunction, high-grade atrioventricular block, myocardial ischemia or infarction, drug effects such as beta-blockers or calcium channel blockers, electrolyte abnormalities like hyperkalemia, hypothyroidism, hypoxia, hypothermia, and increased vagal tone.
❓ How is symptomatic bradycardia diagnosed?
Diagnosis is based on clinical symptoms combined with ECG findings showing bradyarrhythmia. Continuous cardiac monitoring, 12-lead ECG, blood pressure measurement, and evaluation for reversible causes are essential.
❓ What symptoms indicate unstable bradycardia?
Symptoms of unstable bradycardia include hypotension, acute altered mental status, ischemic chest discomfort, syncope, signs of shock, and acute heart failure.
❓ What is the first-line drug for symptomatic bradycardia?
Atropine given intravenously is the first-line medication for most cases of symptomatic bradycardia with a pulse, unless contraindicated or ineffective due to high-grade conduction block.
❓ When is atropine ineffective in bradycardia?
Atropine is often ineffective in Mobitz type II atrioventricular block, complete heart block, and bradycardia due to infranodal conduction disease or severe hypothermia.
❓ When is transcutaneous pacing indicated?
Transcutaneous pacing is indicated in patients with symptomatic bradycardia who are hemodynamically unstable and do not respond to atropine or when atropine is contraindicated or unlikely to be effective.
❓ What infusion drugs are used if pacing is not available?
Dopamine or epinephrine intravenous infusions may be used as temporary measures to increase heart rate and blood pressure when pacing is unavailable or while preparing for pacing.
❓ How is drug-induced bradycardia managed?
Management includes stopping the offending drug, providing supportive care, administering atropine if symptomatic, and using specific antidotes or advanced therapies in cases of overdose.
❓ What role do electrolytes play in bradycardia?
Electrolyte disturbances, especially hyperkalemia, can cause severe bradycardia and conduction blocks. Correction of the electrolyte abnormality is the definitive treatment.
❓ Is bradycardia always pathological?
No, bradycardia can be physiological, such as in well-trained athletes or during sleep, and does not require treatment unless symptoms or hemodynamic compromise are present.
❓ When is a permanent pacemaker required?
A permanent pacemaker is indicated in patients with symptomatic sinus node dysfunction, Mobitz type II atrioventricular block, complete heart block, or recurrent symptomatic bradycardia not due to reversible causes.
❓ What investigations are required after stabilization?
Investigations include continuous ECG monitoring, serum electrolytes, renal function tests, thyroid function tests, cardiac biomarkers if ischemia is suspected, and echocardiography to assess structural heart disease.
❓ Can symptomatic bradycardia recur after initial treatment?
Yes, recurrence is common if the underlying cause is not corrected, which is why definitive treatment such as pacemaker implantation may be necessary in recurrent or persistent cases.